“My Urogynecologist Said Prolapse is Putting my Kidneys at Risk”
My core mission in life is teaching women (and a few good men) about the anatomy of the female body so we can arm ourselves against the dangerous and mistaken practices of the women’s “healthcare” system.
I’ve been speaking with women on the phone and in groups since 2003, researching women’s health since the early 1990’s, and have seen a lot come and go.
One of the tactics urogynecologists have used for the past decade to get women to consent to surgery, is telling them that a prolapsed bladder or uterus is putting strain on their kidneys. Women are terrified because they’ve been told they are at risk of kidney failure.

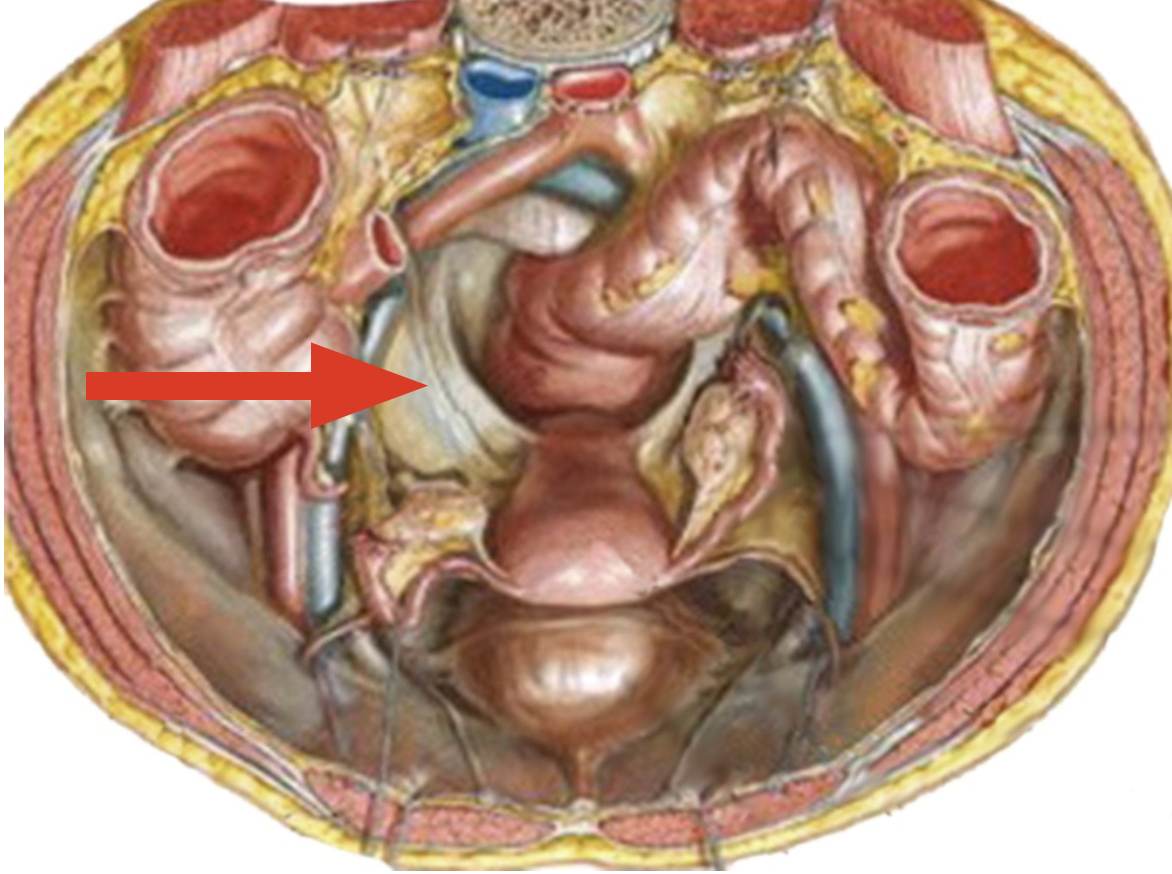
Umbilical ligament
First of all, let’s look at the inside of the abdominal wall. The strong umbilical ligament completely surrounds the front and top of the bladder (red arrow), traveling up the abdominal wall to connect the liver, and ultimately feeding into the respiratory diaphragm. The top, front, and sides of the bladder are held firmly in place. No matter how prolapsed the bladder is, there is no possible way it can fall out.
The ureters, which bring urine down from the kidneys to the bladder, are positioned at the sides of the bladder, not the front, back, or center.
If the bladder is tightly connected to the abdominal wall, how then does bladder prolapse occur?
In normal anatomy, a sharp right angle exists between the urethra (the tube through which urine exits the body), and bladder. This acts like a kink in a garden hose to prevent urinary incontinence.

Cystocele bulge
When women chronically pull their belly in, sit in soft furniture, or other positions that flatten lumbar curvature, intraabdominal pressure (created every time we breathe in) causes the back bladder wall to form a bulge that pushes into the vaginal space.
That bulge can become the size of a half grapefruit, retaining urine, contributing to the development of UTI (bladder infection), and causing general discomfort. However, the bladder itself is still tightly adhered to the abdominal wall.
*Importantly* the ureters are nowhere near the bulging back bladder wall.
The same is true for uterine prolapse. The uterus can be dangling from its round ligaments at or beyond the vaginal opening, but it is not impeding the ureters in any way.
Uterosacral ligaments
What puts the ureters and kidneys at great risk is uterosacral ligament suspension, the most commonly “uterus-sparing” surgery performed for uterine prolapse.
The uterosacral ligaments are not ligaments at all, but tough, stretchy bands of connective tissue surrounding the sides of the bladder, sides of the uterus, and sides of the rectum (red arrow). This connective tissue lines the bony birth canal of the pelvis, separating and securing the organs to the pelvic sidewalls.
The ureters, as well as important nerves, travel through these so-called ligaments, and must be carefully avoided during the surgery. Common “side-effects” of the operation include ureter injury, and chronic pain down the back of the thighs due to damaged nerves.
Urogynecologists have a true conflict of interest with their patients. This is why only the most dangerous, and least effective, surgeries have become the standard of care for prolapse and incontinence.